Liver Cancer Samples
Table of Contents
Introduction | Classification | Diagnosis and Treatment | Considerations for Researchers seeking liver cancer samples | References
Looking for human liver cancer samples for use in research? Contact us for a consultation.
Introduction
Liver cancer, when referred to as such, is any cancer that starts in the liver. Usually when cancer is found in the liver it is cancer that has metastasized from elsewhere in the body. If that is the case, then it is called secondary liver cancer and is characterized based on its point of origin. This article will deal with primary liver cancer, called simply liver cancer.
Liver cancer is the 13th most common cancer according to the SEER fact sheet (National Cancer Institute, 2015). This indication represents about 2.2% of all new cancer cases in the US. Even though relatively few individuals are diagnosed with liver cancer every year, the number of deaths is high because the five-year survival rate for liver cancer is only 17.2% (Ibid.). According to the American Cancer Society, it is estimated that in 2015 there will be over 35,000 new cases of primary liver cancer in the U.S., and that more than 24,000 people would die from the disease. Importantly, liver cancer is much more common in many other parts of the world—in some countries in sub-Saharan Africa and Southeast Asia it is the most common type of cancer, and worldwide it is one of the leading causes of cancer deaths, being responsible for more than 600,000 deaths globally every year. Additionally, the number of new liver cancer cases in the United States has been increasing at an average of 4.0% each year over the last ten years (National Cancer Institute, 2015).
Causes and Risk Factors
For hepatocellular carcinoma (HCC), which is by far the most common type of liver cancer (see “Classification” below), risk factors include:
- Age – The average age at diagnosis is 63, and more than 95% of individuals diagnosed are 45 or older.
- Gender – The ratio of male to female, across all races in the United States, diagnosed with liver and intrahepatic bile duct cancer is roughly 3:1.
- Race/ethnicity – Asian Americans and Pacific Islanders in the United States have the highest rates of liver cancer.
- Chronic viral hepatitis – Infection with hepatitis B or C virus (HBV or HCV) is the most common risk factor for liver cancer worldwide.
- Cirrhosis – Individuals with cirrhosis have an increased risk of developing liver cancer. Alcohol abuse, chronic HBV or HCV infections, some autoimmune diseases, and some types of inherited metabolic diseases can all cause cirrhosis.
- Alcohol abuse – Is the leading cause of cirrhosis, and, hence, a risk factor for developing liver cancer.
- Smoking
- Obesity
- Type 2 diabetes
- Inherited metabolic diseases
- Hereditary hemochromatosis – can lead to cirrhosis and liver cancer through an iron buildup in the liver; one of the most common genetic disorders in the US
- Other rare diseases such as tyrosinemia, glycogen storage diseases, alpha1-antitrypsin deficiency, porphyria cutanea tarda, and Wilson’s disease
- Aflatoxins – made by a fungus that can contaminate peanuts, wheat, soybeans, groundnuts, corn, and rice. The United States and other developed countries regulate the content of aflatoxins in foods by testing. Long-term exposure to aflatoxins is a major risk factor for developing liver cancer.
Classification
Types of liver cancer
Hepatocellular carcinoma (HCC) – HCC is the most common type of liver cancer comprising about 80% of primary liver cancers (American Cancer Society, 2015). HCC is most often caused by cirrhosis of the liver that is itself most commonly caused by alcoholism and hepatitis C in the United States. Because it frequently does not cause symptoms in its earlier stages, it is often not diagnosed until it is in a later stage (Emory Healthcare, 2015). This is one of the factors that can make it difficult to obtain early stage liver cancer samples, but FFPE HCC tumor blocks from excisions performed at later stages of the disease should be available. There are several histological subtypes of HCC, but most of those subtypes do not affect the treatment or prognosis of the disease. It has two different growth patterns:
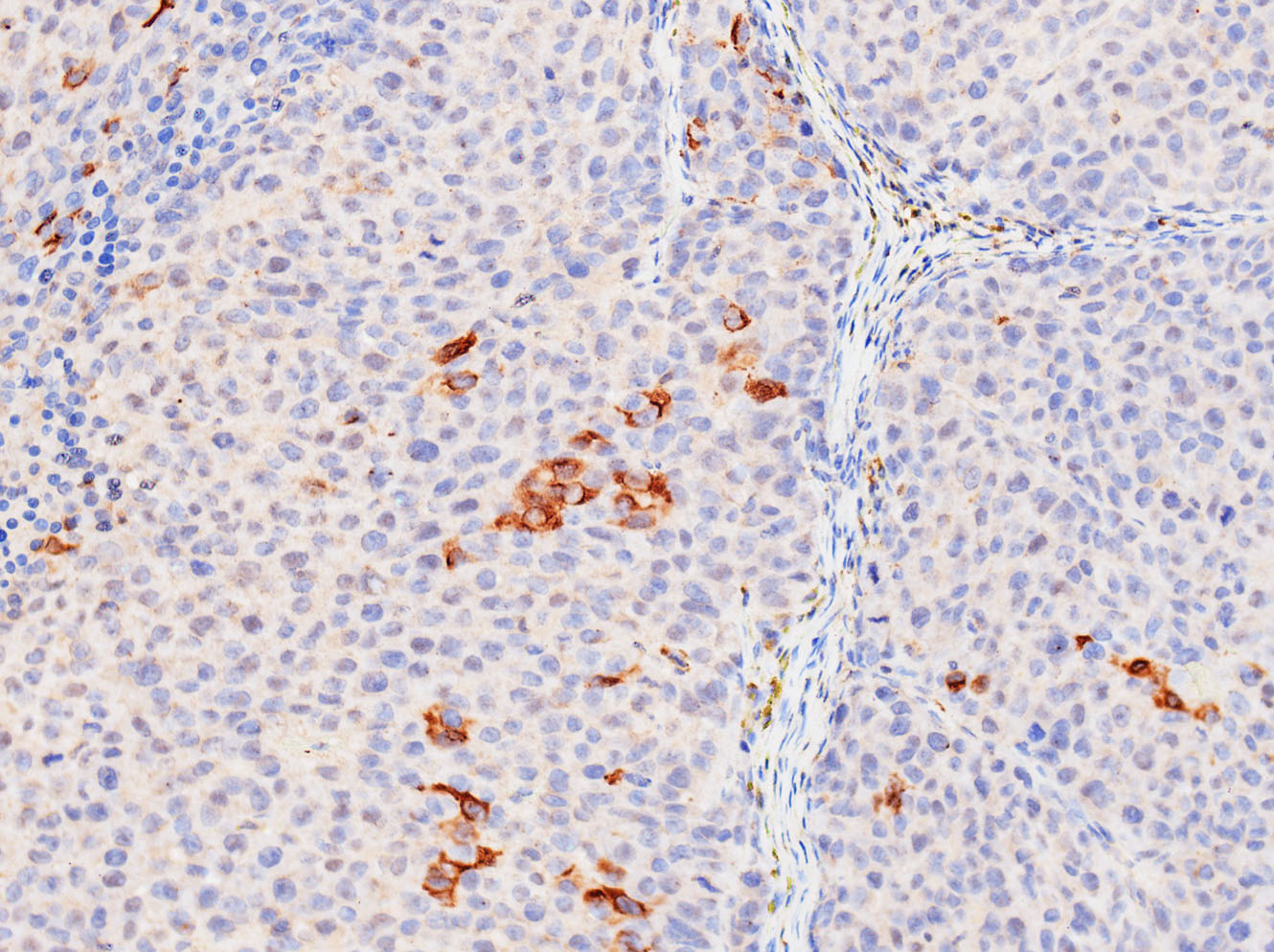
Liver cancer with hepatitis C
- It can begin as a single tumor that gradually grows larger and only spreads to other parts of the liver late in the disease.
- Another growth pattern, and the most common one in the United States, is when HCC starts as many small cancer nodules spread throughout the liver. This type of growth pattern is most often seen in individuals with cirrhosis.
Intrahepatic cholangiocarcinoma (bile duct cancer) – This kind of cancer is responsible for about 10- 20% of primary liver cancers (American Cancer Society, 2015). It is an aggressive form, difficult to cure, that begins in the cells that line the small bile ducts within the liver. Most cholangiocarcinomas, however, actually begin in the bile ducts that lie outside the liver.
Other rare types – Angiosarcoma and hemangiosarcoma are two rare liver cancers that are also very hard to treat; hepatoblastoma is a very rare liver cancer that develops in children who are typically less than four years old.
Staging
TNM staging is used for liver cancer; it describes:
- (T) – the number and size of the primary tumor(s)
- (N) – the extent of spread to regional lymph nodes
- (M) – whether the cancer has metastasized or not
Once the cancer is TNM staged it will be further classified into stages I – IV as with other cancers.
Child-Pugh Score
Another staging system that is used in patients who have cirrhosis is the Child-Pugh score, which is a measure of liver function. There are five factors that are assessed, and then the functionality of the liver can be placed into one of three classes: A, in which liver function is normal; B, in which liver function is mildly abnormal; and C, in which there are severe abnormalities. Patients with class C cirrhosis and liver cancer are frequently too sick to undergo surgery or other primary cancer treatments. The five factors of the Child-Pugh score are:
- Bilirubin blood levels
- Albumin blood levels
- Prothrombin time – how well the liver is producing blood clotting factors
- Whether there is fluid in the abdomen
- Whether the cirrhosis is affecting brain function
The first three of those factors are assessed through blood tests.
Barcelona Clinic Liver Cancer Staging System
The Barcelona Clinic Liver Cancer (BCLC) Staging System is also commonly used to predict the patient’s chance of recovery and plan treatment. It is based on the following:
- The extent of spreading of the cancer—whether it has spread only within the liver or to other parts of the body
- Liver function
- The patient’s health and wellness
- The symptoms the cancer is causing
It is staged as:
- Stage 0 – very early
- Stage I – early
- Stage II – intermediate
- Stage III – advanced
- Stage IV – end-stage
Key Genes and Mutations
The following table is an abridged version of “Table 2: Candidate driver genes in hepatocellular carcinoma with recurrent genetic alterations” from the review article “Exploration of liver cancer genomes” (Shibata & Aburatani, 2014):
| Gene | Frequency (%) | Genetic alteration | Pathway |
|---|---|---|---|
| TP53 | 31 | mutation, LOH | TP53 |
| ARID1A | 28.2 | mutation, LOH | chromatin modifying |
| CTNNB1 | 18.8 | mutation | WNT |
| MTDH | 14.7 | amplification | cell adhesion |
| AXIN1 | 14.2 | mutation, LOH | WNT |
| CDKN2A | 11.7 | mutation, LOH | cell cycle |
| ARID2 | 10.9 | mutation, LOH | chromatin modifying |
| CHD1L | 10.7 | amplification | chromatin modifying |
| BCL9 | 8.7 | amplification | chromatin modifying |
| NFE2L2 | 7.4 | mutation | oxidative stress |
| ATM | 6.9 | mutation, LOH | TP53 |
| PIK3CA | 6.3 | mutation | growth factor signaling |
| SMARCA4 | 6.2 | mutation, LOH | chromatin modifying |
| TSC2 | 5.2 | mutation, LOH | growth factor signaling |
| CCND1 | 4.7 | amplification | cell cycle |
| APC | 4.7 | mutation, LOH | WNT |
| JAK2 | 4.7 | mutation | growth factor signaling |
Other genes and mutations worth mentioning that are not described in the table include the following:
TERT – promoter mutation
TERT is a gene involved in telomere maintenance. Mutations to the TERT promoter have been observed in as much as 60% of HCCs (Schulze, et. al. 2015). These appear early on in HCC carcinogenesis and lead to activation of telomerase expression. Telomerase activation is required for the infinite replication of cancer cells (Shibata and Aburatani, 2014).
RPS6KA3
Mutations in RPS6KA3 have been observed in 7% of HCCs. The result is activation of the RAS-MAPK pathway and increased levels of phosphorylated ERK1 and ERK2. Thus, HCCs that exhibit RPS6KA3 mutations may be targetable with ERK (or MEK) inhibitors (Schulze, et al., 2015).
KEAP1 (associated with NFE2L2)
Mutations in KEAP1 can activate the oxidative stress pathway, which has sometimes been found to be activated in HCCs. Schulze, et al. (2015) found that two out of three cell lines with KEAP1-inactivating mutations were highly sensitive to HSP90 inhibitors.
MLL family: KMT2A/MLL, MLL3, MLL4
Mutations in MLL (also known as KMT2A), MLL3, and MLL4, have been found to recur frequently in HCCs. They are involved in epigenetic regulation (Schulze, et al., 2015, Shibata and Aburatani, 2014).
miRNA
Many HCC mutations are loss-of-function mutations, which means that they cannot easily be targeted for therapy. Genes exhibiting loss-of-function mutations do not make good therapeutic targets for cancers because the restoration of lost gene activity is more difficult to achieve than blocking genes that are overactive in cancer cells (Ozen, et al., 2013). For this reason, many researchers have turned to investigating miRNA as potential therapeutic targets for HCC as several studies have revealed aberrant expression of specific miRNA in HCC cells and tissues. Because miRNA regulate the expression of different oncogenes and tumor suppressor genes (and thus play a role in regulating biological processes such as cellular differentiation, proliferation, and apoptosis), their expression is normally tightly regulated. Their aberrant expression can, then, play a role in carcinogenesis (Morishita and Masaki, 2015).
Studies have found that certain miRNAs are often down-regulated in HCC—miRNAs that may function as tumor suppressors. When the normal expression of tumor suppressive miRNAs is restored, cell cycle block, increased apoptosis, and reduced tumor angiogenesis and metastasis result. There are up- regulated miRNAs in HCC as well—onco-miRNAs that potentially target tumor suppressive genes (Khare, et al., 2013).
- miRNA that have been found to be downregulated in HCC include miR-let-7g, miR-22, miR-26, miR-29, miR-99a, miR-122, miR-124, miR-139, miR-145, and miR-199b.
- miR-126, miR-27b, miR-182, miR-183, miR-199, miR-200a, miR-214, and miR-322 have been found to be downregulated in alcohol-related HCC.
- miRNA that have been found to be upregulated in HCC include miR-10b, miR-17-5p, miR-21, miR-135a, miR-155, miR-182, miR-221, and miR-222 (Morishita and Masaki, 2015).
Diagnosis and Treatment
Liver cancer can be challenging to diagnose. Liver cancer is usually symptomless in its early stages, and liver tumors often cannot be felt from outside. There are, however, several tests that will help determine if an individual has liver cancer:
- Blood tests – the alpha-fetoprotein blood test is a common blood tests that can detect alpha- fetoprotein (AFP), which can be an indicator of liver cancer. Other blood tests may be run to check how well the liver is functioning or for signs of viral hepatitis.
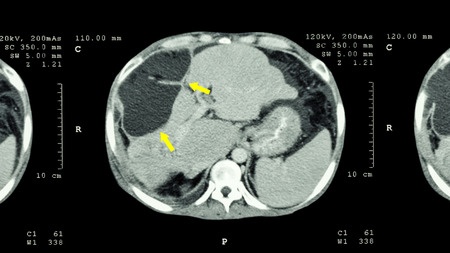
- Imaging tests
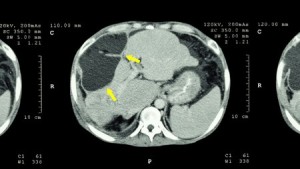
CT scan of upper abdomen, showing abnormal mass at the liver.
- MRI
- CT scan
- Ultrasound
- Angiography – blood vessels injected with dye for X-ray visibility
- Biopsy
- Fine needle aspiration (FNA)
- Core biopsy
- Surgical biopsy
- Laparoscopy – a thin lighted tube and camera are inserted for viewing; a tissue sample
may or may not be taken
Current Treatments & Targeted Therapies
Treatment options for liver cancer include surgery to remove part of the liver, liver transplant, tumor ablation, tumor embolization, radiation therapy, targeted therapy, and chemotherapy. The therapies administered to an individual patient will depend primarily on the stage of liver cancer, health of the liver, and overall health of the patient. Instead of using TNM staging to provide direction for the course of therapy, however, physicians classify liver cancers as: potentially resectable or transplantable, unresectable, inoperable with only local disease, or advanced. Details regarding the treatment options are as follows.
- Resection – Resection is the standard treatment If the liver is healthy and the tumor is in an early stage. While in the US only 5% of patients diagnosed with liver cancer will qualify for resection, a 60-75% 5-year survival rate can be achieved. By five years post-resection, however, 70% of patients will have recurrent HCC (Waghray, et al., 2015).
- Transplant – Due to the scarcity of livers available for transplant, there are certain qualifications for patients to be considered candidates for liver transplant. There are three different scoring criteria used to determine eligibility, but in general, the tumor(s) must be small (early stage) and the liver in poor condition. There is a four-year survival rate of 85% for patients who undergo liver transplant who meet the criteria (Waghray, et al., 2015).
- Tumor ablation – Chemical or thermal ablation can be used to treat liver cancers that are not resectable and which have neither spread to lymph nodes nor metastasized. Radiofrequency ablation (RFA, a type of thermal ablation) is superior to the standard form of chemical ablation, but the efficacy of RFA decreases with increasing tumor size (Waghray, et al., 2015, American Cancer Society, 2015).
- Transarterial chemoembolization (TACE) – Patients who are not candidates for resection or transplant and whose tumors are too large for ablation may undergo TACE, in which the blood supply to the tumor is shut off and the area is treated with chemotherapy (Waghray, et al., 2015).
- Chemotherapy & Radiation – Both chemotherapy and radiation can be used in the treatment regimen for liver cancer patients. Liver cancers, however, are resistant to most chemotherapy drugs, showing either little response or a response that does not last long. (American Cancer Society, 2015)
- Targeted therapies – Sorafenib, an anti-angiogenic tyrosine kinase inhibitor, is the standard of care for treating patients with advanced stage HCC. It is also the only systemic therapy so far found to be effective for treating advanced stage HCC (Waghray, et al., 2015).
Trends in Standard Care Looking Forward
Several avenues of research are underway to find new and better treatments for liver cancer. Some studies revolve around improving surgical treatment by studying adjuvant therapies (administered directly after surgery to minimize the chance of the cancer recurring) or neoadjuvant therapies (administered prior to surgery to try to shrink the tumor(s) so as to make them resectable) (American Cancer Society, 2015).
Immunotherapy, alone or in combination with other therapies, is also being studied for improvements in cancer treatment. There are several different types of immunotherapy: checkpoint inhibitors/immune modulators, therapeutic vaccines, adoptive T cell transfer, monoclonal antibodies, cytokines, and oncolytic virus therapy. Most of the drugs/agents in these therapies that are being studied are currently in phase I or II clinical trials. Checkpoint inhibitors/immune modulators, often antibodies, are designed to cause the patient’s own immune system to mount an attack on the cancer cells. Therapeutic vaccines are designed to cause the immune system to respond to tumor-associated or tumor-specific antigens. Adoptive T-cell therapy is an approach in which T-cells are removed from the patient, then treated with chemicals or genetically modified in order to enhance their activity, and then introduced back into the patient in an attempt to enhance the immune system’s anti-cancer activity. Monoclonal antibodies generated in the lab, target specific tumor antigens. Cytokines play a role in controlling the growth and activity of immune system cells. Oncolytic virus therapy causes tumor cells to self-destruct by using a virus modified to specifically infect tumor cells (Cancer Research Institute, 2014).
Considerations for Researchers Seeking Liver Cancer Samples
Because so few liver cancer patients in the United States qualify for surgical resection, liver cancer samples may be hard to come by, especially for later stage liver cancers. Samples may be available from biopsies because of their use in diagnoses.. Blood samples may also be available as they too can be involved in the diagnosis of liver cancer. Keep in mind, however, that scientists need to be realistic about requesting volumes greater than 1 ml, custom collection protocols, or anything else that deviates from standard care. The more your collection requirements deviate from standard care, the harder the request will be to fill.
For liver cancer samples collected prospectively, plan ahead as collection times can exceed several months depending on your inclusion and exclusion criteria. Biomarker information is only available if it was collected as part of standard care at the time of treatment. Data mining fees may apply if you require knowledge of specific biomarker criteria that were tested for as part of standard care. Remember that many biorepositories and biobanks contain primarily FFPE samples that have been CAP graduated, which means that elapsed time since the collection procedure often exceeds ten years, and data associated with the samples will reflect standard care as it was a decade ago. Biomarker screening of samples by us is possible, but this is unlikely to be cost effective unless you want to purchase all tested specimens regardless of their biomarker profile. If you only want samples with certain markers, you will have to pay for testing of the ones that are negative too. A better alternative may be to purchase sections only for a statistically suitable number of cases, screen them in your own lab using your preferred assay or a third-party, high volume genetic screening service, then request the blocks of interest.
References
- American Cancer Society (2015). Liver Cancer. Retrieved from http://www.cancer.org/cancer/livercancer/detailedguide/index.
- Cancer Research Institute (November 2014). Liver Cancer. Retrieved from http://www.cancerresearch.org/cancer-immunotherapy/impacting-all-cancers/liver-cancer.
- Emory Healthcare (2015). Malignant Liver Tumors. Retrieved from http://www.emoryhealthcare.org/liver/liver-diseases/malignant-liver-tumors.html.
- Khare, S., Zhang, Q., & Ibdah, J. A. (2013). Epigenetics of hepatocellular carcinoma: Role of microRNA. World Journal of Gastroenterology : WJG, 19(33), 5439–5445. http://doi.org/10.3748/wjg.v19.i33.5439
- Memorial Sloan Kettering Cancer Center (2015). Liver Cancer: Risk, Prevention & Screening. Retrieved from https://www.mskcc.org/cancer-care/types/liver/risk-factors-prevention.
- Morishita, A., & Masaki, T. (February 01, 2015). miRNA in hepatocellular carcinoma. Hepatology Research, 45, 2, 128-141.
- National Cancer Institute (2015). SEER Stat Fact Sheets: Liver Cancer. Retrieved from http://seer.cancer.gov/statfacts/html/livibd.html.
- Ozen, C., Yildiz, G., Dagcan, A. T., Cevik, D., Ors, A., Keles, U., Topel, H., … Ozturk, M. (January 01, 2013). Genetics and epigenetics of liver cancer. New Biotechnology, 30, 4, 381-4.
- Schulze, K., Imbeaud, S., Letouzé, E., Alexandrov, L. B., Calderaro, J., Rebouissou, S., Couchy, G., … Zucman-Rossi, J. (January 01, 2015). Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nature Genetics, 47, 5, 505-11.
- Shibata, T., & Aburatani, H. (January 01, 2014). Exploration of liver cancer genomes. Nature Reviews. Gastroenterology & Hepatology, 11, 6, 340-9.
- The University of Texas MD Anderson Cancer Center (2015). Liver Cancer Diagnosis. Retrieved from
http://www.mdanderson.org/patient-and-cancer-information/cancer-information/cancer-types/liver-cancer/diagnosis/index.html. - Waghray, A., Murali, A. R., & Menon, K. N. (May 18, 2015). Hepatocellular carcinoma: From diagnosis to treatment. World Journal of Hepatology, 7, 8, 1020-9.
- Zhang, Z. (January 01, 2012). Genomic landscape of liver cancer. Nature Genetics, 44, 10, 1075-7.