Bladder Cancer Samples
Table of Contents
Introduction | Classification |Risk Factors | Diagnosis and Treatment | Considerations for Researchers seeking bladder cancer samples | References
Looking for human bladder cancer samples for use in your research? Contact us for a consultation.
Introduction
Urinary bladder cancer is the 9th most common type of cancer worldwide and the 4th most common type of cancer among men. An estimated 74,000 new cases were diagnosed in the US during 2015. Over 550,0000 people in the US have a history of bladder cancer including those who no longer have the disease (American Cancer Society). An estimated 16,000 deaths from bladder cancer occurred in 2015 with the median age of death at 79 (SEER). Bladder cancer affects almost 4 times more men than women and occurs twice as often in white males as compared to black males (American Cancer Society). The development of transurethral surgeries has made procurement of early bladder cancer samples more feasible than it was 10 years ago, but these samples tend to be small.
Classification of Bladder Cancer
Subtypes of Bladder Cancer
Bladder cancer is categorized based on individual cell characteristics as well as the progression of the disease into the lining of the bladder wall (American Cancer Society).
Transitional Cell Carcinoma (TCC): The most prevalent type of bladder cancer is transitional cell carcinoma (TCC) and is the source of more than 9 in 10 cases of bladder cancer. Because TCC’s affect the urothelial cells, which are found in the walls of bladder, ureters, urethra and kidneys, this cancer may occur in any or all of these places (American Cancer Society). TCC’s are the second most common cause of death in patients from genital and urinary (genitourinary) tumors (Vardar, 2006). Transitional cell carcinomas (TCC’s) are further divided into the following two categories:
- Papillary carcinomas: These cancers present as finger-like projections that grow from the walls of the urinary system outward into the structural centers. Papillary carcinomas tend to occur superficially and have low lethality due to their tendency to grow away from the structural walls rather than invading the muscle tissue and metastasizing.
- Flat Carcinomas:By contrast, flat carcinomas form as flat cells in the layer closest to the center of the bladder and can be characterized as non-invasive flat carcinoma or a flat carcinoma in situ (CIS)(American Cancer Society). The latter may result in metastatic disease with possible recurrence or death (Vardar, 2006).
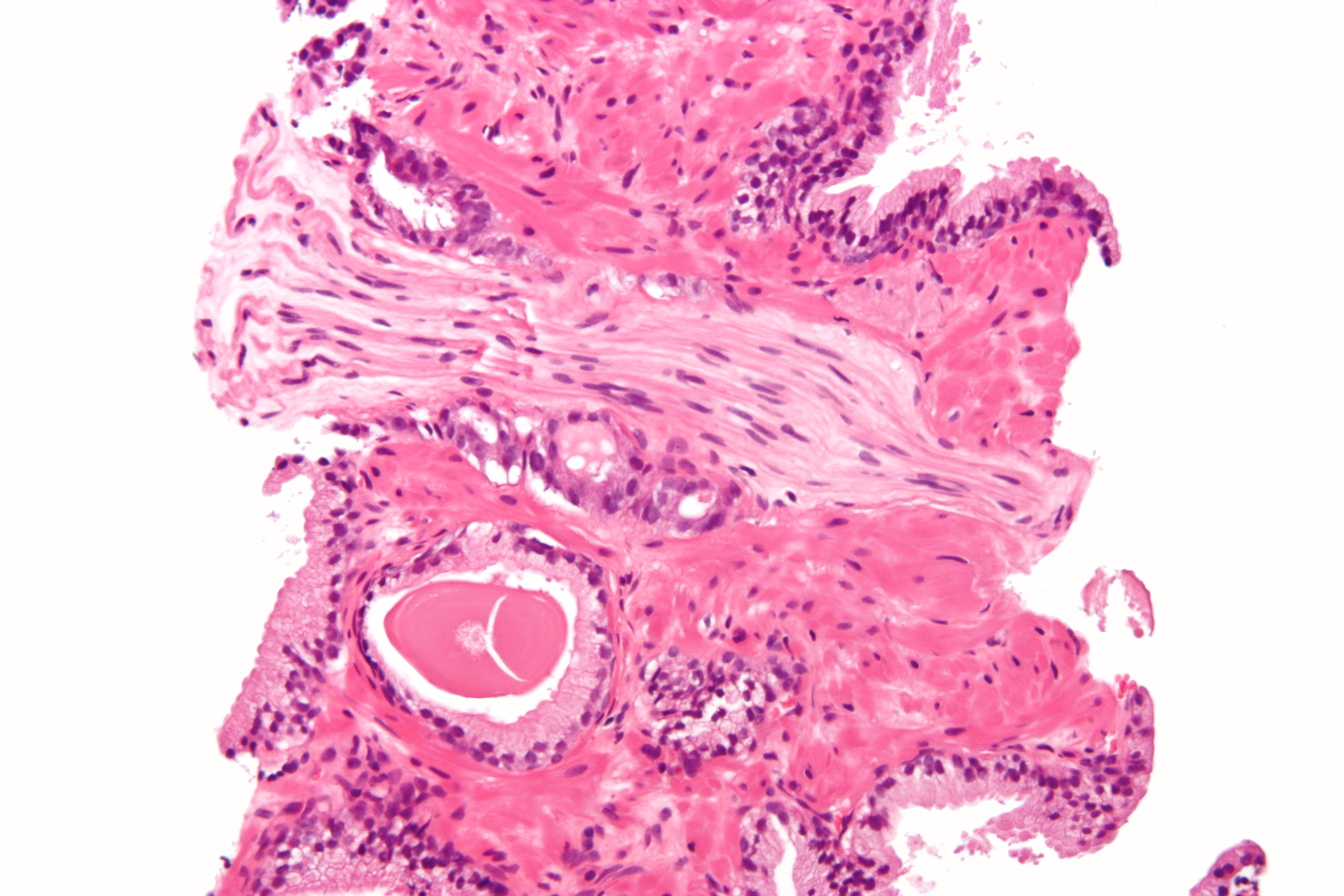
Prostatic adenocarcinoma with perineural invasion
Squamous Cell Carcinoma: This type of bladder cancer is much less common at between 1% and 2% of all bladder cancer cases. Most cases of squamous cell carcinomas are invasive.
Adenocarcinomas: Adenocarcinomas make up only about 1% of bladder cancers and almost all cases of this type are invasive.
Small Cell Carcinoma: This type of cancer occurs in the neuroendocrine cells and grows fairly rapidly. Less than 1% of bladder cancers are of this type.
Sarcoma: This type of cancer is the rarest of the bladder cancers and begins in the muscle cells of the bladder (American Cancer Society). Sarcoma is malignant and therefore highly lethal (Sarcoma Foundation of America).
Stages:
Stages are used by physicians to describe the growth and spread of cancer in a standardized way.
The layers of the bladder wall are important in identifying the stage of cancer development and are listed below followed by the stages of bladder cancer:
- Bladder lining
- Connective tissue
- Muscle
- Fat
- Stage 0a: Cancer that is limited to the surface or inner lining of the bladder. Cancer of this stage can usually be removed easily. This stage of cancer describes noninvasive papillary urothelial carcinoma.
- Stage 0is: This stage is similar to 0a, and involves the surface of the bladder, but involves carcinoma in situ (CIS).
- Stage I: Cancer that has grown through the inner layer, but has not yet reached the muscle tissue, or other organs.
- Stage II: Cancer that has spread into the muscle wall. This is called muscle invasive cancer and has not yet reached the layer of fatty tissue in the bladder.
- Stage III: Cancer that has reached the layer of fatty tissue surrounding the muscle wall. It may also have spread to the prostate in men, or the uterus and vagina in women.
- Stage IV: Cancer that has spread beyond the fatty tissue to other organs, but may or may not have reached the lymph nodes. (Cancer.Net)
Risk Factors
Smoking
Cigarette smokers are three times more likely to develop bladder cancer than non-smokers (Maurice, 2002). Gender differences in smoking habits may account for some of the disparity in bladder cancer rates among men and women.
Gender
Men are 3 to 4 times more likely to develop bladder cancer in their lifetime than women. Although some of this discrepancy may be explained by differenced in smoking habits, and exposure to chemicals due to occupational differences, the most likely reason for the observed differences in bladder cancer rates is due to hormonal differences in men and women. Specifically, the presence of BHP (the hormone responsible for prostate growth) and associated urinary symptoms increase as men age. (Michaud, 2007)
Age
Bladder cancer affects the elderly with 90 percent of patients diagnosed over the age of 55 and the median age diagnosed at 73. (Cancer Treatment Centers of America)
Exposure to Chemicals
Aromatic amines (used in pesticides, pharmaceuticals and dyes), cyclophosphamide (used in the treatment of certain cancers and nephrotic syndrome) and analgesic phenacetin have been implicated in increasing the risk of developing bladder cancer. (Michaud, 2007)
Diagnosis and Treatment
Treatment Options
Surgery
Transurethral surgery may be appropriate for early-stage or superficial bladder cancers. This is the least invasive type of surgery and involves the removal of the tumor without cutting into the abdomen. Unfortunately, patients with transurethral surgery often experience a reoccurrence of the cancer after the original tumor has been removed.
A second type of surgery called a cystectomy involves the complete or partial removal of the bladder. This type of surgery is used mainly for cancers that have invaded the muscle tissue. Often, the removal of the prostate in men, or the removal of the uterus, ovaries, fallopian tubes and a small portion of the vagina in women is also required.
Intravesical Therapy
Two types of intravesical therapies may be used for treatment of bladder cancer:
- Intravesical Immunotherapy: This type of therapy uses microorganisms or interferon to stimulate the immune system. A promising type of intavesical therapy is BCG therapy in which bacillus Calmette-Guérin bacterium is administered into the bladder (Medscape).
- Intravesical Chemotherapy: This treatment involves the insertion of chemotherapy drugs into the bladder to kill actively growing cancer cells.
Chemotherapy
Chemotherapy can be local or systemic. Local chemotherapy involves the deposition of drugs directly into the affected region. Systemic chemotherapy occurs when the drug is ingested to be absorbed into the bloodstream, or injected directly into the circulatory system.
Cisplatin-based neoadjuvent chemotherapy has been shown to increase survival rate of patients with muscle invasive bladder cancer. Chemotherapy increasingly starts as soon as the cancer is diagnosed, so researchers need to have realistic expectations about the likelihood of obtaining pre-treatment bladder cancer samples.
Radiation Therapy
Radiation therapy involves the use of high-energy radiation to shrink or kill cancer cells. Often, radiation therapy is used in combination with other types of therapies.
Please see http://www.cancer.org/cancer/bladdercancer/detailedguide/bladder-cancer-treating-general-info for more extensive information on any of the above treatment options.
Standard of Care
Diagnosis
Cystoscopy is considered the best resource in the diagnosis of bladder cancer. Bladder cancer is rarely diagnosed postmortem due to the clinical presentation of the disease. MRI and CT scans have low sensitivity to the cancer and additional testing may be required if bladder cancer is suspected. Surveillance of early stage bladder cancer after treatment is required. Approximately 50% of patients initially diagnosed with high-grade bladder cancer already have invasive disease. After a cystectomy, examination of 9 lymph nodes is sufficient for assessment of the bladder cancer stage.
Treatment
Non-invasive tumors (Ta) and tumors in-situ (T1) are treated by the direct removal of the cancerous tissue from the bladder (transurethral resection), with recurrence rate as high as 50-70%. If the cancer reappears, the physician may perform another transurethral resection. This process may occur several times before more extreme treatment measures are considered. Because non-invasive tumors and tumors in-situ are so commonly resected, bladder cancer samples of this type will often be available. 10-20% of patients who undergo transurethral resection procedures alone will eventually have the cancer progress to an invasive stage. Transurethral resection in combination with intravesical BCG therapy results in a better outcome than transurethral resection alone. Approximately 20% of non-invasive tumors can be removed through surgery without recurrence of the cancer (far less than the recurrence rate with transurethral resection alone) and only about 10-30% of these eventually progress to invasive disease. Flat carcinomas are diagnosed at the superficial stage approximately 70% of the time and progress to invasive disease in about 5-10% of these cases. Therefore, samples of flat carcinoma bladder cancer that has progressed to the invasive form of the disease may be harder to come by. Most deaths due to bladder cancer are attributed to invasive stages of the disease.
The standard treatment for invasive bladder cancer is a cystectomy with removal of all tissue within the genitofemoral nerve laterally, the bladder medially, the circumflex iliac vein inferiorly (known as the lymph node of Cloquet), the bifurcation of the common iliac artery superiorly, and the hypogastric blood vessels posteriorly. Because much of the tissue removed is normal, samples of both normal and diseased tissue from the same patient will commonly be available. Several different types of tissue, including lymphatic tissue, within the resected area may also be available from the same patient. The general prognosis of patients undergoing this treatment is poor with the majority of these patients dying of metastases within 3 years.
Relevant Findings
Mutations in HRAS and FGFR3 are linked to low grade non-invasive papillary tumors. Invasive Bladder cancers have been linked to mutations or deletions in tumor suppressor genes, including TP53, Rb and PTEN. Telomerase activity is detected in all superficial urothelial cancer cells.
Please see http://standardofcare.com/Bladder_cancer for more information on standard of care.
Considerations for Researchers
Common treatments for patients with bladder cancer include surgery, therefore FFPE bladder cancer samples and frozen bladder cancer samples will commonly be available. The treatment for non-invasive bladder cancer often includes the removal of the diseased tissue from the inner lining of the bladder only, or precise microsurgery using new trans-urethral techniques. Therefore, only diseased tissue may be available from these patients with only small amounts of normal adjacent tissue (NAT) being excised.
For bladder cancer samples collected prospectively, plan ahead as collection times can exceed several months depending on your inclusion and exclusion criteria. Biomarker information is only available if it was collected as part of standard care at the time of treatment. Data mining fees may apply if you require specific biomarker criteria. Remember that many biorepositories and biobanks contain primarily FFPE samples that have been CAP graduated, which means that they are at least ten years old, and data associated with the samples will reflect standard care as it was a decade ago.
Biomarker screening of samples is possible, but this is unlikely to be cost effective unless you want to purchase all tested specimens regardless of their biomarker profile. If you only want samples with certain markers, remember that you will have to pay for testing of the ones that are negative too. A better alternative may be to purchase sections only for a suitable number of cases, screen them in your own lab using your preferred assay, then request the blocks of interest.
References
American Cancer Society. Bladder Cancer. 02 25 2015. 03 02 2016
http://www.cancer.org/cancer/bladdercancer/detailedguide/bladder-cancer-what-is-bladder-cancer.
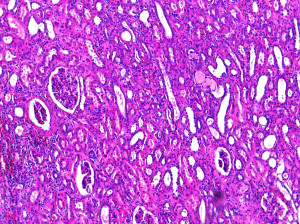
Bladder Urothelial Carcinoma CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=507416
Cancer Facts and Figures 2015. Atlanta: American Cancer Society, 2015.
Cancer Treatment Centers of America. Bladder Cancer risk Factors. 06 02 2016
http://www.cancercenter.com/bladder-cancer/risk-factors/.
Cancer.net. Bladder Cancer: Stages and Grades. 06 2015. 06 02 2016
http://www.cancer.net/cancer-types/bladder-cancer/stages-and-grades.
Maurice, P, et al. “A Prospective Study on Active and Enviornmental Tobacco
Smoking and Bladder Cancer.” Cancer Causes and Control 13.1 (2002): 83-
90.
Medscape. Bacillus Calmette-Guerin Immunotherapy for Bladder Cancer Overview
of BCG Immunotherapy. 12 05 2014. 11 02 2016 http://emedicine.medscape.com/article/1950803-overview.
Michaud, Dominique. “Chronic Inflammation and Bladder Cancer.” Urologic
Oncology: Seminars and Original Investigations 25.3 (2007): 260-268.
National Cancer Institute. Bladder Cancer Treatment. 01 07 2015. 11 02 2016
http://www.cancer.gov/types/bladder/patient/bladder-treatment-pdq.
SEER Stat Fact Sheets: Bladder Cancer. 11 02 2016
http://seer.cancer.gov/statfacts/html/urinb.html.
Pasin, E, et al. “Superficial Bladder Cancer: An Update on Etiology, Molecular
Developement, Classification, and Natural History.” Reviews in Urology 10
(2008): 31-43.
Prostatic Adenocarcinoma with Perineural Invasion Nephron – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=10552036
Razmaria, Aria. “Bladder Cancer.” The Journal of the American Medical Association
314.17 (2015).
Sarcoma Foundation of America. Patient Resources . 2016. 03 02 2016
http://www.curesarcoma.org/patient-resources/.
Standard of Care. Bladder Cancer. 04 11 2015. 11 02 2016
http://standardofcare.com/Bladder_cancer.