Prostate Cancer Samples
Table of Contents
Introduction | Causes and Risk Factors | Classification | Key Genes and Mutations | Diagnosis and Treatment | Considerations for Researchers | References
Looking for human prostate cancer samples for use in your research? Contact us to discuss your needs.
Introduction
Prostate cancer is the second most common cancer among men, with about 1 out of every 7 men diagnosed during his lifetime. In 2012 more than 177,000 men in the US were diagnosed with prostate cancer, and the estimated number of diagnoses for 2015, according to the SEER fact sheet, was 220,800 (National Cancer Institute, 2015). The good news is that most of the men who are diagnosed with prostate cancer do not die from it; the five-year survival rate is 98.9%. Part of the reason for this is that many prostate tumors are very slow growing and may need no treatment (Mayo Clinic, 2015). Additionally, the death rate has been falling by an average of 3.5% each year, documented over the years 2003-2012, so that the estimated number of deaths for 2015 was less than 28,000. The rate of new prostate cancer cases diagnosed has also been falling, by 4.3% per year on average over the last ten years. These trends have a number of implications for the procurement of FFPE, fresh and frozen prostate cancer samples. Once prostate cancer has metastasized, survival is very limited (National Cancer Institute, 2015).
Causes and Risk Factors
The causes of most prostate cancers are not well known. There are some inherited genetic mutations that seem to cause a small percentage of prostate cancers, but the majority of prostate cancers appear to arise from mutations that develop over a man’s lifetime. Known genetic mutations that can be inherited include mutations of the following genes: BRCA1, BRCA2, RNASEL, and HOXB13 (tumor suppressor genes); and DNA mismatch repair genes such as MSH2 and MLH1. Such inherited mutations appear to cause about 5-10% of all prostate cancers (Genetics Home Reference, 2015; American Cancer Society, 2015; Xu, et al. 2013).
Risk factors for prostate cancer include the following:
- Age: Prostate cancer is rarely diagnosed in men under the age of 40. The median age of diagnosis is 66, and most prostate cancers are diagnosed between the ages of 64 and 75 (National Cancer Institute, 2015).
- Race/Ethnicity: Black males are more often diagnosed with prostate cancer than males of any other race or ethnicity, and they are more than twice as likely as white males to die from it (Prostate Cancer Foundation, 2015).
- Genetics and Family History: As mentioned above; additionally, several risk-related chromosomal loci have been identified to be over-transmitted from parents to affected offspring in hereditary prostate cancer families with several affected members (Jin, et al. 2012). This highlights the fact that the hereditary component of prostate cancer has not yet been entirely elucidated.
- Diet: Men who eat a lot of red meat and/or high fat dairy products, and also fewer fruits and vegetables, appear to be at higher risk of developing prostate cancer, although it is not certain whether it might be the lack of fruits and vegetables or the large amount of red meat and/or high fat dairy products that could be to blame (American Cancer Society, 2015).
- High grade prostatic intraepithelial neoplasia (HGPIN): The presence of high grade PIN appears to confer a risk of developing prostate cancer – a 26.3% risk according to one study (Hou, et al. 2011). Other studies also indicate that HGPIN can be a precursor to prostate cancer (De Nunzio, et al. 2009; Montironi, et al. 2011).
Classification of Prostrate Cancer
Types of Prostate Cancer
Histological
Acinar adenocarcinoma is by far the most common type of prostate cancer, comprising more than 90% of all prostate cancer diagnoses. It originates from gland cells in the prostate and typically grows slowly and does not spread. There are other types of adenocarcinomas than acinar, but those are treated in the same way as acinar adenocarcinoma. The other prostate cancers, less than 10% of those diagnosed, are the following:
- Ductal adenocarcinoma: often grows and spreads more quickly than acinar adenocarcinoma, so it is sometimes already in advanced stage by the time it is diagnosed
- Transitional cell (or urothelial) carcinoma: usually starts in the bladder and spreads into the prostate
- Squamous cell cancer: like ductal adenocarcinoma, tends to grow and spread more quickly than acinar adenocarcinoma so is sometimes already advanced by the time it is diagnosed; does not cause an increase in prostate specific antigen (PSA)
- Carcinoid: begins in cells of the neuroendocrine system; very rare and may be slow growing
- Small cell cancer: a type of neuroendocrine tumor and an aggressive form that is often advanced by the time it is diagnosed; does not cause an increase in prostate specific antigen (PSA)
- Sarcomas and sarcomatoid cancers: sarcomas develop from muscle cells and often grow quickly; sarcomatoid cancers have both sarcoma and adenocarcinoma cells
(Cancer Research UK, 2014; Cancer Research Society, 2010)
Molecular
A recently published study found another way to differentiate prostate cancers, based not on histological architectures but molecular signatures instead. The researchers distinguished five integrative subgroups with characteristic molecular profiles. They called them iClusters and numbered them 1 – 5. iCluster 1 and 3 exhibited consistent copy number loss (DNA deletions) and downregulation of gene expression. iCluster 3 also showed significant copy number gain (DNA repetitions) and upregulation of certain genes. These two subgroups were associated with the highest risk of relapse. Two of the subgroups, iCluster 2 and 4, had relatively few changes in copy number or gene expression and were also associated with the best outcomes. iCluster 5 had more copy number alterations than iCluster 2 and 4 but fewer copy number alterations than iCluster 1 and 3 (Ross-Adams, et al. 2015).
Another study published in 2015 (Robinson, et al.) is being called the “Rosetta Stone” for prostate cancer as it has led to significant insights regarding the particular genetic aberrations of an advanced form of the disease, different pathways they affect, and potential individualized treatments for patients with advanced stage prostate cancer. The study revealed distinct molecular subtypes of metastatic castration-resistant prostate cancer (mCRPC) (an aggressive form of prostate cancer that does not respond to androgen therapy). More information is provided below under “Key Genes and Mutations.”
Stages
Prostate cancer is a multifocal cancer, meaning that more than one tumor or tumor nodule can arise in the prostate, in different areas. Studies have indicated that a high percentage of prostates with cancer possess two or more separate tumors by the time of diagnosis. These different tumor foci can progress at different rates depending on the specific genetic alterations within them. Because of this multifocality, accurate staging of prostate cancer is often challenging to accomplish (Andreoiu and Cheng, 2010). Nevertheless, there are classification systems in place that help healthcare practitioners assign a stage to a patient’s prostate cancer.
Like other cancers, prostate cancer is staged using the TNM staging system where T describes the local extent of the cancer, N describes whether the cancer has spread into regional lymph nodes, and M describes the extent of metastasis if any. Once the cancer has been TNM staged, that information will be combined with the measured levels of prostate-specific antigen (PSA) and the Gleason score. The Gleason score is determined by a pathologist based on the appearance of the cancer cells in tissue following biopsy or surgery. Cancer cells that are similar in appearance to healthy cells are given a low score, and the more poorly differentiated the cells are the higher the score will be (American Society of Clinical Oncology, 2014). Using these three pieces of information and classification, the cancer will be further classified as stage I, II, III, or IV:
- Stage I: the cancer can or cannot be felt, it is in half or less of one side of the prostate, the Gleason score is 6 or less, and the PSA level is less than 10.
- Stage II: the cancer has not yet spread outside the prostate—neither to regional lymph nodes nor elsewhere in the body. However, either the Gleason score or PSA level (or both) is higher than stage I if the cancer is classified as stage II, or it is in both sides of the prostate.
- Stage III: the cancer has grown outside the prostate, at most into the seminal vesicles, and has neither invaded the lymph nodes nor metastasized. The Gleason score and PSA level can be any value.
- Stage IV: the cancer has spread to tissues next to the prostate—other than the seminal vesicles—yet has not spread into lymph nodes and has not metastasized; or it may or may not have spread into tissues next to the prostate but has spread into the lymph nodes and has not metastasized; or it has metastasized, with or without spreading into lymph nodes or regional tissues. The Gleason score and PSA level can be any value (American Cancer Society, 2015).
Key Genes and Mutations
Some of the genes more frequently implicated in prostate cancer include the following:
- PTEN: Phosphatase and tensin homologue tumor suppressor gene; research indicates that deletions in PTEN can contribute to some prostate cancers (Robinson, et al. 2015; Barbieri, Demichelis, and Rubin, 2012; Hughes, et al. 2005).
- NKX3.1: This tumor suppressor gene can be lost in chromosomal deletion of the 8p12-21 region. Loss of 8p is thought to occur early on in prostate cancer carcinogenesis, occurring in as much as 80% of prostate tumors (Shen & Shen, 2000). A significant percentage of PIN lesions, low and high stage prostate cancers, and androgen independent prostate cancers have all been found to lack the NKX3.1 gene. Its absence has been discerned in a high percentage of prostate cancer metastases as well, and it has also been found to be hypermethylated in some prostate cancers (Reynolds, 2008; Hughes, et al. 2005).
- AR: Amplifications, somatic mutations, and epigenetic modifications can occur in the androgen receptor (AR) gene in prostate cancer. The reactivation of this gene, by any of those means, is a key event in the development of hormone-refractory prostate cancer. Somatic mutations of AR have also been shown to be more common in metastatic samples than in primary samples of prostate cancer (Barbieri, Demichelis, and Rubin, 2012; Reynolds, 2008).
- MYC: Amplifications of this oncogene have been identified in prostate cancers (Barbieri, Demichelis, and Rubin, 2012; Reynolds, 2008; Hughes, et al. 2005).
- p53: The tumor suppressor gene p53 is often implicated in various cancers. In prostate cancer, p53 mutations occur less frequently in early stages and more frequently in advanced stages as well as in recurrent and metastatic prostate cancers. The overall frequency of p53 mutations in prostate cancer is about 20-30% (Reynolds, 2008; Hughes, et al. 2005; Shen & Shen, 2000).
- SPOP: Mutations in the SPOP gene, which encodes the substrate-recognition component of a Cullin 3-based E3-ubiquitin ligase, have been identified in 6-13% of prostate cancers. SPOP mutations were, however, only found in prostate cancer tumors that were negative for ERG rearrangement (see below) which suggests that tumors with SPOP mutations represent a distinct molecular class of prostate cancers (Barbieri, Demichelis, and Rubin, 2012).
- PCA3: – PCA3 is a prostate-specific gene that is overexpressed in more than 95% of prostate cancers. The non-coding RNA that it codes for is useful as a biomarker, and a urine test has been developed that checks for excessive levels of it (Barbieri, Demichelis, and Rubin, 2012).
ETS Gene Fusions
Gene fusions are common in cancers, and in prostate cancer the most common gene fusion is TMPRSS2-ERG, which has been identified as present in about 50% of prostate cancers (Kumar-Sinha, Tomlins, and Chinnaiyan, 2008). ERG (ETS-related gene) is a transcriptional regulator; fusion with TMPRSS2 results in “androgenic induction of oncogenic transcription factor overexpression,” (Witte, 2009). TMPRSS2 fusions occur with other ETS family genes, but those account for a minority of the prostate cancer gene fusions (Witte, 2009).
The “Rosetta Stone” of Prostate Cancer
A study published in 2015 (Robinson, et al.) is being called the “Rosetta Stone” for prostate cancer as it has led to significant insights regarding different genetic aberrations of the disease, different pathways they affect, and potential individualized treatments for patients with advanced stage prostate cancer. The study revealed distinct molecular subtypes of metastatic castration-resistant prostate cancer (mCRPC) based on alteration clustering and biological pathways. Genes involved in the AR pathway, WNT pathway, PI3K pathway, DNA repair, the cell cycle, and chromatin modifier gene sets, among others, were implicated in mCRPC. The genes found to be most often aberrant in mCRPC included AR (62.7%), ETS family genes (56.7%), TP53 (53.3%), and PTEN (40.7%). Moreover, the study found that nearly 90% of mCRPC patients possessed a clinically actionable aberration, meaning there may be current drugs or investigational drugs that could treat a patient’s own unique mCRPC. As such, this study represents a breakthrough in the understanding and treatment potential of advanced stage prostate cancer.
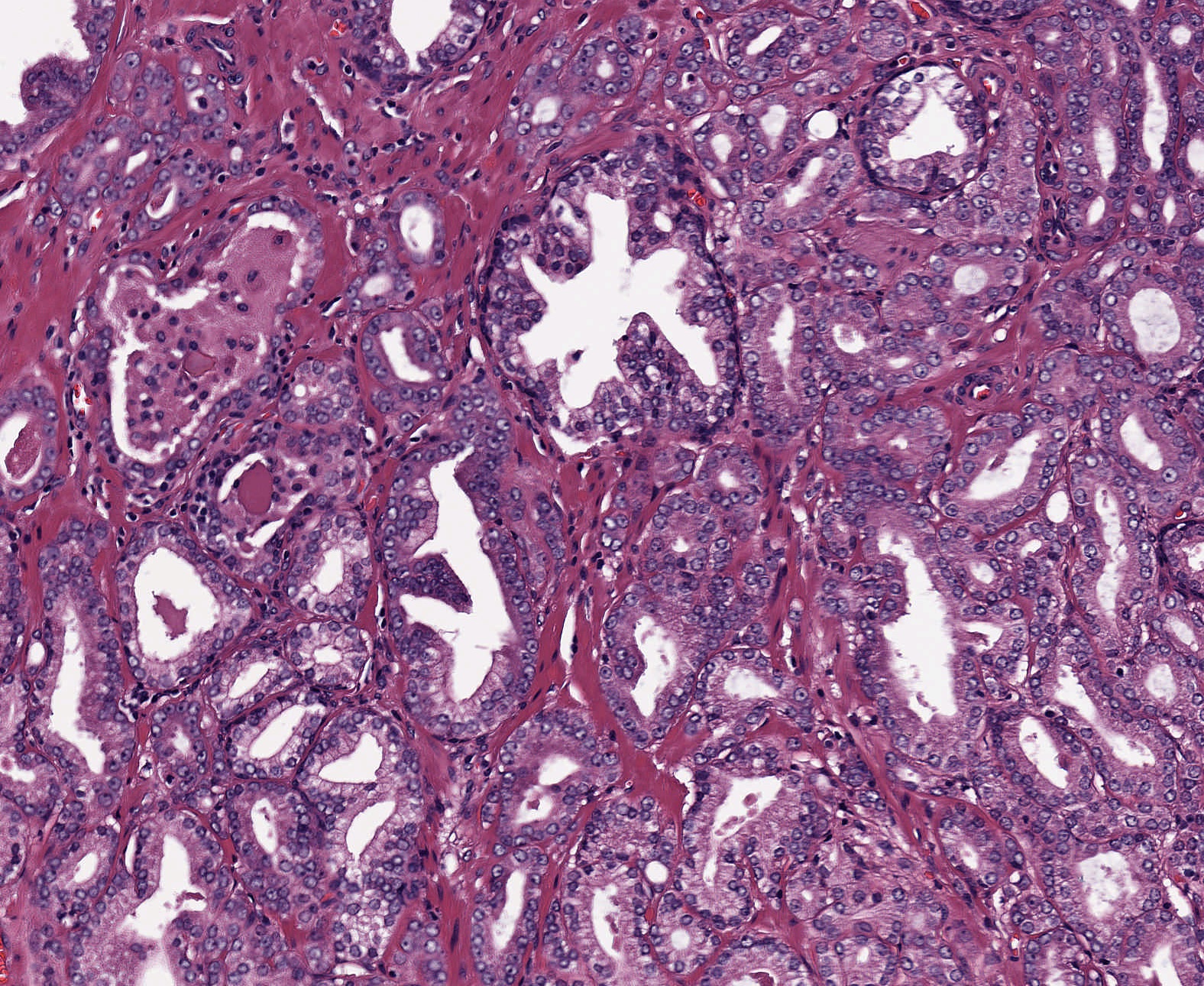
Prostatic adenocarcinoma, involved left and right lobes.
Diagnosis and Treatment
Diagnosis
A digital rectal exam (DRE) and prostate-specific antigen (PSA) blood test are typically involved in the diagnosis of prostate cancer. Biopsy and transrectal ultrasound (TRUS) can also indicate the presence of prostate cancer. Normally, twelve tissue samples will be taken during a biopsy, but there is still the potential that cancer may be missed if the needle does not intersect with any cancer that may be present. The PSA blood test is also not definitive but often useful in diagnosis. If PSA levels are below 4 ng/mL, it is unlikely that the individual has prostate cancer. As PSA levels rise, the likelihood of there being cancer in the prostate rises as well: when PSA levels are between 4 and 10 ng/mL there is a 25% chance of cancer, and when they are above 10 ng/mL there is a 50% chance of prostate cancer (American Cancer Society, 2015). Normal PSA levels are, however, not well established (Barbieri, Demichelis, and Rubin, 2012). Additionally, a urine test has been developed to detect the presence of the ncRNA product of the PCA3 gene which is highly overexpressed in most prostate cancers, as mentioned above, but as this is a newer test it may or may not be utilized in a given office or clinic. A bone scan, CT scan, MRI, ProstaScint™ scan, and, occasionally, lymph node biopsy may be used after prostate cancer has been diagnosed to check for spreading.
Biomarkers
There are a variety of biomarkers to choose from in the diagnosis and prognosis of prostate cancer using biopsy samples, some of which are in current use, and some of which may not yet have progressed past investigation. These include, but are not limited to, the following, as described in the review “Diagnostic and prognostic molecular biomarkers for prostate cancer” (Kristiansen, 2012):
- Basal cell markers: basal cell cytokeratins and p63: prostate cancers are characterized by loss of basal cells, so testing for basal cell markers has become an integral part of prostate cancer diagnosis. Only very rarely do prostate cancers still express them.
- Alpha-methylacyl-CoA racemase (AMACR): upregulated in most prostate cancers, this enzyme has gained clinical acceptance as a biomarker, and in combination with basal cell markers it can increase diagnostic accuracy. There are drawbacks associated with it, however, so alternative diagnostic biomarkers may be in some cases more useful.
- GOLM1: a protein overexpressed in most prostate cancers, it can be helpful in identifying prostate cancers in AMACR-negative cases. Its expression in benign tissues makes it somewhat unsuitable for evaluation of suspicious glands, however.
- FASN: the protein product of this gene is overexpressed in prostate cancer, and as AMACR-negative prostate cancers are usually positive for FASN, it could potentially be a useful biomarker.
- ERG: as mentioned above, TMPRSS2-ERG gene fusions are present in about 50% of prostate cancers. This causes a truncated ERG product to be overexpressed in those cancers. Antibodies for it have made it available as a diagnostic marker, so it may be useful in some cases.
- PSA, Prostein, NKX3.1, and ERG: all could be useful to demonstrate prostatic origin of cancers. AR is not recommended for that purpose.
- PITX2, Ki-67, and certain miRNAs (e.g. miR-96 and miR-221): these could be useful as prognostic biomarkers for prostate cancer. miRNAs are relatively stable and can be analyzed in FFPE samples. PITX2 hypermethylation is associated with poor prognosis. Ki-67 is a protein that has also been associated with poor prognosis.
Current Treatment and Therapies
Localized Cancer Treatments
As is common with cancers, treatment options vary depending on the stage and severity of prostate cancer. If the cancer is “indolent,”—unlikely to cause symptoms, spread, or shorten a patient’s life—then a physician may recommend active surveillance with the DRE, PSA test, ultrasound, and biopsy at regular intervals. Other treatment options for localized prostate cancer include radical prostatectomy, in which the entire prostate is removed along with some of the surrounding tissue, including the seminal vesicles. Lymph nodes around the prostate may be removed as well. Radiation therapy and focal therapies are other options for treating prostate cancer. Radiation therapy often is as effective at treating early-stage prostate cancer as is radical prostatectomy. It can also eliminate more aggressive local tumors, provide long-lasting remission, and treat bone metastases (Memorial Sloan Kettering Cancer Center, 2015).
Systemic Therapies
There are a few treatment options for advanced prostate cancers, cancers that have spread beyond the prostate:
- Hormone (Androgen Deprivation) Therapy This therapy can shrink and slow the growth of prostate tumors, even those that have metastasized. It is commonly used for advanced prostate cancers, yet in the end the cancer can recur in a highly aggressive androgen independent form—castrate-resistant or hormone-refractory prostate cancer (Shen & Shen, 2000).
- Chemotherapy Sometimes given to individuals with advanced stage prostate cancer.
- Immunotherapy In which a patient’s immune system cells are harvested, engineered to fight the prostate cancer cells, and returned to the body.
mCRPC Therapies
The standard of care therapies for metastatic castration-resistant prostate cancer (mCRPC), for which androgen deprivation therapy (ADT) is not effective, include docetaxel, abiraterone, and enzalutamide, all of which confer a survival benefit to affected individuals yet none of which is curative (Petrioli, et al. 2015; Robinson, et al. 2015). A number of targeted therapies have not proven effective for mCRPC in phase III clinical trials, while others may yet hold potential. Petroli, et al. (2015) provide a review of some of the most recent experimental targeted therapies for mCRPC.
Trends in Standard Care Looking Forward
While most experimental targeted therapies in the past have fallen short for providing survival advantages or curative effects for mCRPC, investigations will likely continue the search for effective drugs. Recently published studies, such as that published by Robinson, et al. (2015), may be instrumental in discovering effective mCRPC therapies, as previously mentioned. For localized prostate cancers, surgery, radiation, and focal therapies are likely to remain standard treatment options along with active surveillance of indolent tumors.
Considerations for Researchers Seeking Prostate Cancer Samples
Due to the prevalence of the disease and the widespread use of prostate biopsies for prostate cancer diagnosis, tissue samples should be readily available to the researcher. Blood samples should also be readily available as they are commonly drawn to determine PSA levels. Keep in mind, however, that scientists need to be realistic about requesting volumes greater than 1 ml, custom collection protocols, or anything else that deviates from standard care. The more your collection requirements deviate from standard care, the harder the request will be to fill.
For prostate cancer samples collected prospectively, plan ahead as collection times can exceed several months depending on your inclusion and exclusion criteria. Biomarker information is only available if it was collected as part of standard care at the time of treatment. Data mining fees may apply if you require knowledge of specific biomarker criteria that were tested for as part of standard care. Remember that many biorepositories and biobanks contain primarily FFPE samples that have been CAP graduated, which means that elapsed time since the collection procedure often exceeds ten years, and data associated with the samples will reflect standard care as it was a decade ago. Biomarker screening of samples by us is possible, but this is unlikely to be cost effective unless you are willing to purchase all tested specimens regardless of their biomarker profile. If you only want samples with certain markers, you will have to pay for testing of the ones that are negative too. A better alternative may be to purchase sections only for a statistically suitable number of cases, screen them in your own lab using your preferred assay or a third-party, high volume genetic screening service, then request the blocks of interest.
References
Abate-Shen, C., & Shen, M. M. (January 01, 2000). Molecular genetics of prostate cancer. Genes & Development, 14, 19, 2410-34.
American Cancer Society (2015). Prostate Cancer. Retrieved from http://www.cancer.org/cancer/prostatecancer/detailedguide/index.
American Society of Clinical Oncology (October, 2014). Prostate Cancer: Stages. Retrieved from http://www.cancer.net/cancer-types/prostate-cancer/stages.
Andreoiu, M., & Cheng, L. (June 01, 2010). Multifocal prostate cancer: biologic, prognostic, and therapeutic implications. Human Pathology, 41, 6, 781-793.
Barbieri, C. E., Demichelis, F., & Rubin, M. A. (January 01, 2012). Molecular genetics of prostate cancer: emerging appreciation of genetic complexity. Histopathology, 60, 1, 187-98.
Cancer Research Society (2010). Types of Prostate Cancer. Retrieved from http://www.crs-src.ca/page.aspx?pid=1801.
Cancer Research UK (February 20, 2014). Types of Prostate Cancer. Retrieved from http://www.cancerresearchuk.org/about-cancer/type/prostate-cancer/about/prostate-cancer-types.
De Nunzio, C., Trucchi, A., Miano, R., Stoppacciaro, A., Fattahi, H., Cicione, A., & Tubaro, A. (January 01, 2009). The number of cores positive for high grade prostatic intraepithelial neoplasia on initial biopsy is associated with prostate cancer on second biopsy. The Journal of Urology, 181, 3, 1069-74.
Genetics Home Reference (November 23, 2015). Prostate Cancer. Retrieved from http://ghr.nlm.nih.gov/condition/prostate-cancer.
Hou, H., Li, X., Chen, X., Wang, C., Zhang, G., Wang, H., Gong, H., … Zhang, X. (January 01, 2011). Prediction value of high-grade prostatic intraepithelial neoplasia for prostate cancer on repeat biopsies. The Chinese-German Journal of Clinical Oncology, 10, 7, 410-414.
Hughes, C., Murphy, A., Martin, C., Sheils, O., & O’Leary, J. (January 01, 2005). Molecular pathology of prostate cancer. Journal of Clinical Pathology, 58, 7, 673-84.
Jin, G., Lu, L., Cooney, K. A., Ray, A. M., Zuhlke, K. A., Lange, E. M., Cannon-Albright, L. A., … International Consortium for Prostate Cancer Genetics. (January 01, 2012). Validation of prostate cancer risk-related loci identified from genome-wide association studies using family-based association analysis: evidence from the International Consortium for Prostate Cancer Genetics (ICPCG). Human Genetics, 131, 7, 1095-103.
Kristiansen, G. (January 01, 2012). Diagnostic and prognostic molecular biomarkers for prostate cancer. Histopathology, 60, 1, 125-41.
Kumar-Sinha, C., Tomlins, S. A., & Chinnaiyan, A. M. (January 01, 2008). Recurrent gene fusions in prostate cancer. Nature Reviews. Cancer, 8, 7, 497-511.
Mayo Clinic (March 03, 2015). Prostate Cancer Definition. Retrieved from http://www.mayoclinic.org/diseases-conditions/prostate-cancer/basics/definition/con-20029597.
Memorial Sloan Kettering Cancer Center (2015). Prostate Cancer Treatment. Retrieved from https://www.mskcc.org/cancer-care/types/prostate/treatment.
Montironi, R., Mazzucchelli, R., Lopez-Beltran, A., Scarpelli, M., & Cheng, L. (January 01, 2011). Prostatic intraepithelial neoplasia: its morphological and molecular diagnosis and clinical significance. Bju International, 108, 9, 1394-401.
National Cancer Institute (2015). SEER Stat Fact Sheets: Prostate Cancer. Retrieved from http://seer.cancer.gov/statfacts/html/prost.html.
Petrioli, R., Francini, E., Fiaschi, A. I., Laera, L., & Roviello, G. (January 01, 2015). Targeted Therapies for Prostate Cancer. Cancer Investigation, 33, 7, 276-85.
Prostate Cancer Foundation (2015). Prostate Cancer Risk Factors. Retrieved from http://www.pcf.org/site/c.leJRIROrEpH/b.5802027/k.D271/Prostate_Cancer_Risk_Factors.htm.
Reynolds, M. A. (November 18, 2008). Molecular alterations in prostate cancer. Cancer Letters, 271, 1, 13-24.
Robinson, D., Van Allen, E. M., Wu, Y.-M., Schultz, N., Lonigro, R. J., Mosquera, J.-M., Montgomery, B., … Chinnaiyan, A. M. (May 21, 2015). Integrative Clinical Genomics of Advanced Prostate Cancer. Cell, 161, 5, 1215-1228.
Ross-Adams, H., Lamb, A. D., Dunning, M. J., Halim, S., Lindberg, J., Massie, C. M., Egevad, L. A., … CamCaP Study Group. (January 01, 2015). Integration of copy number and transcriptomics provides risk stratification in prostate cancer: A discovery and validation cohort study. Ebiomedicine, 2, 9, 1133-44.
Witte, J. S. (January 01, 2009). Prostate cancer genomics: towards a new understanding. Nature Reviews. Genetics, 10, 2, 77-82.
Xu, J., Lange, E. M., Lu, L., Zheng, S. L., Wang, Z., Thibodeau, S. N., Cannon-Albright, L. A., … International Consortium for Prostate Cancer Genetics. (January 01, 2013). HOXB13 is a susceptibility gene for prostate cancer: results from the International Consortium for Prostate Cancer Genetics (ICPCG). Human Genetics, 132, 1, 5-14.