Stomach Cancer Samples
Table of Contents
Introduction | Classification | Diagnosis and Treatments | Considerations for Researchers | References
Looking for human stomach cancer samples for use in research? Contact us for a consultation.
Introduction
Stomach cancer, also called gastric cancer (GC), is the 15th most common cancer in the United States. According to the SEER fact sheet, the estimated number of new stomach cancer cases for 2015 was 24,590—which was also expected to be 1.5% of all new cancer cases—and the estimated number of deaths from stomach cancer for 2015 was 10,720, or about 1.8% of all cancer deaths (National Cancer Institute, 2015b). Additionally, it was estimated in 2012 that in the United States there were nearly 77,000 people living with the disease. The prevalence worldwide, however, is much higher, for which it is estimated to be the fourth leading cause of cancer and the second-leading cause of cancer deaths. In 2012 alone, 952,000 new cases were diagnosed throughout the world (Gastric Cancer Foundation, 2015; Torre et al., 2015; World Cancer Research Fund International, 2015).
Stomach cancer also has a high mortality rate, largely owing to the fact that it is often not diagnosed until it is in a later stage. In the US, while the numbers of both new cases and deaths from GC have been falling over the last few decades, death rates did not change significantly over the years 2002-2012 (National Cancer Institute, 2015b). The five-year relative survival rate, though, has increased to approximately 29.3% currently from 14.3% in 1975 (Ibid.).
Causes & Risk Factors
Causes and risk factors for developing stomach cancer include:
- Helicobacter pylori infection – H. pylori infection is considered the primary cause of stomach cancer although the majority of infections do not lead to stomach cancer. H. pylori is a bacterium that dwells in the mucus layer of the stomach and can cause infection there.
- Age – Stomach cancer is most common in the elderly; the average age of those who are diagnosed with stomach cancer is 69, and about 60% of those who are diagnosed with stomach cancer are 65 or older.
- Gender – Men are more often diagnosed with stomach cancer than women; the ratio of men to women of all races who get stomach cancer is about 10.1:5.3 in the U.S., but varies widely between countries. In Eastern Asian countries, such as China, Japan, Korea, and Mongolia, the incidence of newly diagnosed cases of stomach cancer is nearly 3 times more common in males than in females. (Torre et al., 2015)
- Diet – Those who consume a diet high in smoked, pickled, and salted foods have an increased risk of developing stomach cancer. Those whose diet contains large quantities of fresh fruits and vegetables have a lower risk of developing stomach cancer.
- Smoking (Tobacco) – Individuals who smoke are twice as likely to develop stomach cancer as non-smokers.
- Previous Stomach Surgery – Those who have had part of their stomach removed are more likely to develop stomach cancer.
- Pernicious Anemia – Causes an increased risk of developing stomach cancer.
- Family History and Genetics – If someone has a first-degree relative (parent, sibling, or child) who has had stomach cancer, then they are at increased risk of developing it as well. There are also inherited genetic disorders that can cause stomach cancer; for instance, Hereditary diffuse gastric cancer is an inherited syndrome that, while rare, increases the risk of stomach cancer in affected individuals by about 70% – 80%.
For a more detailed list of genetic/inherited and other risk factors, see “What are the risk factors for stomach cancer?” at http://www.cancer.org/cancer/stomachcancer/detailedguide/stomach-cancer-risk-factors.
Classification
Types of Stomach Cancer

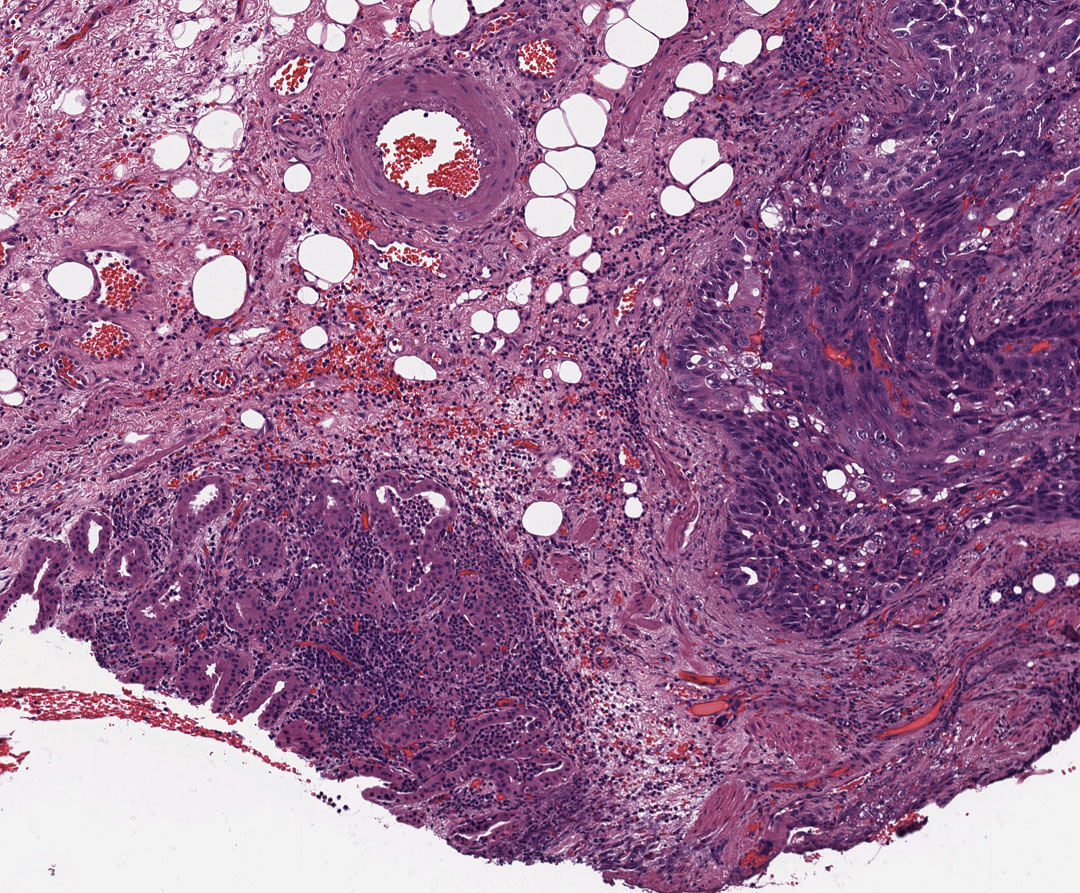
Sample from an esopho-gastrectomy, of mucinous adenocarcinoma, gastroesophageal junction.
- Adenocarcinoma – About 90-95% of all stomach cancers are of this type and therefore the greatest availability of stomach cancer samples will be for this indication. Adenocarcinomas develop from the stomach mucosa (its innermost layer) that is composed of glandular tissue. There are two main types of gastric adenocarcinoma:
- Intestinal type – closely associated with dietary and environmental factors such as a diet high in salt and H. pylori infection. It is characterized by the formation of gland-like structures, and its pathogenesis is considered to be a “long-term multistep progression from chronic gastritis to chronic atrophy to intestinal metaplasia to dysplasia,” (Hudler, 2012) a process that is sometimes called the Correa pathway. It is dependent on chronic inflammation.
- Diffuse type – less common than the intestinal type but more common in younger patients. It can also arise in part from H. pylori infection but without the intermediate steps such as gastric atrophy and intestinal metaplasia. Its histological characterization is of poor differentiation and a lack of glandular structures. The prognosis is usually worse than with the intestinal type.
- Lymphoma – Comprising about 4% of all stomach cancers, lymphomas develop in immune system tissue within the stomach wall.
- Others – Gastrointestinal stromal tumor (GIST), Carcinoid tumors, and other rare cancers can also develop in the stomach.
Stages of Stomach Cancer
The stomach wall has five layers, and they are involved in the determination of the stage of stomach cancer (discussed below) as stomach cancer often begins in the innermost layer (mucosa) and advances into the deeper, or outer, layers. The five layers, from innermost to outermost are:
- Mucosa – where digestive enzymes and stomach acid are synthesized
- Submucosa – supportive of the mucosa
- Muscularis propria – muscular layer, enables churning of the stomach contents
- Subserosa
- Serosa
The stages of stomach cancer are determined by combining information from TNM staging into Stages I-IV and further subdivided based on where exactly the cancer has spread to.
- Stage 0 – The cancer has not grown past the inner layer of cells lining the stomach; this is its earliest stage.
- Stage I – Cancer has formed in the mucosa (the innermost layer of the stomach wall). It may have spread further into the submucosa or even the muscularis propria. Spreading to one or two lymph nodes may have occurred as well.
- Stage II – Cancer has advanced into the submucosa and several lymph nodes; or the muscularis propria and a few lymph nodes; or it has advanced into the subserosa or serosa, possibly in combination with spreading into one or two lymph nodes as well. Overall, the cancer will have spread deeper into the stomach wall and/or to more lymph nodes than a stage I cancer.
- Stage III – Cancer has spread into the muscularis propria, serosa, or subserosa as well as lymph nodes, or it has spread to nearby organs and possibly lymph nodes. Overall, the cancer will have spread deeper into the stomach wall and/or to more lymph nodes than a stage II cancer.
- Stage IV – Cancer has metastasized (spread to distant parts of the body).
Genetics of Stomach Cancer
Gastric cancer is incredibly complex and heterogeneous, and the detailed mechanisms of the genetic changes that lead to its development remain uncertain, although it is clear that gastric carcinogenesis is a multistep process that involves different genetic and epigenetic changes in many different genes as well as an individual’s genetic background and environmental factors. However, most gastric adenocarcinomas are characterized by genetic instability, either microsatellite instability (MSI) or chromosomal instability (CIN), both of which play a large part in gastric carcinogenesis.
Chromosomal Instability (CIN)
The most common type of genomic instability in solid tumors is chromosomal instability. It is characterized by gain or loss of whole chromosomes (aneuploidy) and/or fractions of chromosomes (loss of heterozygosity (LOH), amplifications, and translocations), all of which alterations can affect the expression of tumor suppressor genes, oncogenes, and other genes such as DNA repair genes. CIN is the most common feature detected in sporadic gastric cancers, and it has been reported in as much as 84% of gastrointestinal tumors (Hudler, 2012). While the genetic mechanisms leading to CIN are still largely unknown, at least three potential mechanisms have been proposed: aberrant expression, mutations and/or polymorphisms in mitotic genes (implicated in chromosome segregation), or the activity of carcinogens in individuals with susceptible genetic backgrounds. Chromosome instability can also arise from H. pylori infection (Hudler, 2012).
Microsatellite Instability (MSI)
Microsatellite instability is a change that occurs in the DNA of cells so that the number of repeats of microsatellites in DNA is different from the original number as found in the parent cell. It is caused by defective repair of DNA replication by mismatch repair genes. Because mismatch repair genes proofread DNA and repair replication errors, inactivation or deficiency of one or more of those genes causes MSI and often leads to frameshift mutations that often cause the loss of a large portion of a protein (Hamilton & Meltzer, 2006). Inactivation of mismatch repair genes in gastric cancer is primarily associated with epigenetic inactivation (CpG island methylator pathway, CIMP). Studies indicate that MSI is characteristic for some hereditary gastric cancers and is also found in 25% to 50% of sporadic gastric cancers (Hudler, 2012). MSI is associated with antral tumor location, intestinal type GCs, and a better prognosis.
Genes Implicated in Gastric Cancer Development
As stated above, gastric cancer is extremely heterogeneous, and the number of altered genes implicated in gastric carcinogenesis is very large. A short list of genes that have been associated with gastric cancer is below.
- APC – mutations of or LOH in this gene have been implicated in GC, especially intestinal type (Hamilton & Meltzer, 2006; Zheng, et al., 2004).
- CDH1 – mutation of this gene is a biomarker of hereditary diffuse gastric carcinoma (HDGC, accounts for a small percentage of all cases of GC), also found in some cases of sporadic gastric cancers. It encodes the protein E-cadherin (Hamilton & Meltzer, 2006).
- COX-2 – found to be frequently upregulated in gastric adenocarcinomas. Its expression is thought to occur early on in gastric carcinogenesis (Milne, et al., 2009).
- HER2/neu – overexpressed in some stomach cancers (American Cancer Society, 2015).
- MLH1 – hypermethylated MLH1 (through the CpG island methylator pathway) is a primary cause of microsatellite instability (MSI) (Hamilton & Meltzer, 2006; Hudler, 2012).
- TP53 – found to be inactivated in over 50% of all cancers, its inactivation plays a significant role in many gastric cancers as well. Loss of heterozygosity (LOH) and mutations are the primary means of its inactivation. Because of the large role it plays in genetic stability—through the p53 protein that it encodes—by regulating the expression of hundreds of genes and noncoding RNAs and triggering responses such as cell-cycle arrest, DNA repair, apoptosis, and by preventing multiplication of damaged cells, its inactivation has been found to be involved in both the early stages and later development of cancer. Thus it can serve as an important biomarker in many cancers, gastric cancers included (Marilanda, et al., 2012).
- Some genes found to have reduced expression in gastric carcinomas include MAD1 and MAD2 (Hudler, 2012).
- Some genes found overexpressed in gastric carcinomas include AURKA, CCNB1, CCNE1, PTTG1, and PLK, all of which are important regulators of cell cycle progression (Hudler, 2012).
In a field-synopsis and meta-analysis conducted in January of 2015 (Mocellin, et al.,), 11 gene variants were found both 1) to be significantly associated with disease risk and 2) to have a high level of summary evidence supporting their involvement in GC. Thus they are high-quality biomarkers of susceptibility to GC, and are listed in the table below.
| Meta-Analysis Data | ||||
| Gene | Variant ID | Chromosomal location | Subgroup | Mutation |
|---|---|---|---|---|
| MUC1 | rs2070803 | 1q22 | diffuse | SNP |
| MTX1 | rs2075570 | 1q22 | diffuse | SNP |
| PSCA | rs2976392 | 8q24.2 | intestinal | SNP |
| PSCA | rs2294008 | 8q24.2 | non-cardia | SNP |
| PRKAA1 | rs13361707 | 5p13 | non-cardia | SNP |
| PLCE1 | rs2274223 | 10q23 | cardia | SNP |
| TGFBR2 | rs3087465 | 3p22 | Asian | SNP |
| PKLR | rs3762272 | 1q22 | diffuse | SNP |
| GSTP1 | rs1695 | 11q13 | Asian | SNP |
| TNF | rs1799724 | 6p213 | mixed | SNP |
| CASP8 | rs3834129 | 2q33 | mixed | deletion |
Diagnosis and Current Treatments
Diagnosis
Primarily because of late onset of clinical symptoms, gastric cancer is often diagnosed at a late stage. There are, however, several tests, scans, and procedures that can be involved in its diagnosis:
- Upper endoscopy
- Endoscopic ultrasound
- X-ray with barium swallow
- CAT scan
- PET scan
- MRI
- Laparoscopy
- Biopsy
- Blood tests
Current Treatments
Surgery, chemotherapy, targeted therapy, and radiation therapy are all used against stomach cancer.
An esophagogastrectomy specimen.
Treatment based on stage:
- Stage 0 – Surgery
- Stage I – Treatment possibilities include: surgery, surgery followed by chemoradiation therapy, or clinical trial of chemoradiation therapy prior to surgery. Surgery—proximal or distal subtotal gastrectomy or total gastrectomy—is standard treatment. Regional lymphadenectomy is recommended in addition to resection. Patients with node-positive (T1 N1) and muscle-invasive (T2 N0) disease may undergo postoperative chemoradiation therapy as well.
- Stage II – Treatment possibilities include: surgery, surgery followed by chemoradiation therapy or chemotherapy, chemotherapy before and after surgery, a clinical trial of surgery followed by chemoradiation therapy that tests new anticancer drugs, or a clinical trial of chemoradiation therapy prior to surgery. As with Stage 1 gastric cancer, surgical resection of the stomach with accompanying regional lymphadenectomy is recommended. Postoperative chemoradiation therapy may be more often administered to patients with Stage 2 GC, however, than to patients with Stage 1 GC.
- Stage III – Radical surgery is standard treatment for patients with Stage 3 GC. Postoperative chemoradiation therapy and both perioperative and postoperative chemotherapy are standard as well.
- Stage IV – Chemotherapy, targeted therapy, radiation therapy, laser therapy, surgery, and clinical trials of new combinations of chemotherapy may all be used as palliative therapies.
For more information, visit: http://www.cancer.org/cancer/stomachcancer/detailedguide/stomach-cancer-treating-by-stage
Targeted therapies:
- Trastuzumab (Herceptin) – a monoclonal antibody, can be used on stomach cancers that exhibit too much of the HER2/neu protein (about 1/5 of stomach cancers); administered via IV.
- Ramucirumab – a monoclonal antibody; used primarily on advanced stomach cancers, usually after another drug stops having an effect; inhibits VEGF from binding to its receptors; administered via IV.
Trends in Standard Care Looking Forward
Targeted Therapies
Drugs that are currently being studied for the effects on stomach cancer include several that block the HER2 protein: lapatinib (Tykerb®), pertuzumab (Perjeta®), and trastuzumab emtansine (Kadcyla®); a drug that blocks the protein EGFR (which is highly expressed in gastric cancer patients): Panitumumab (Vectibix®); and a variety of other targeted drugs, ones that target different parts of cancer cells, such as sorafenib (Nexavar®) and apatinib (National Cancer Society 2015a).
For more information, visit: http://www.cancer.org/cancer/stomachcancer/detailedguide/stomach-cancer-new-research.
Immunotherapy
About 9% of gastric cancers test positive for Epstein-Barr virus (EBV), in which cancers the PD-L1/2 ligand is found to be overexpressed (Bass, et al., 2014). Pembrolizumab is a monoclonal antibody that blocks the interaction between the PD-1 receptor on T-cells and its ligands PD-L1 and PD-L2 expressed on cancer cells that trigger apoptosis of the T-cells upon binding and thus enable the cancer cells to evade the immune system (Matsueda & Graham, 2014; Morano, et al., 2015). In a phase 1B study, anti-tumor activity of Pembrolizumab was observed (Muro, et al., 2014). Other drugs that target this interaction are also being investigated.
Considerations for Researchers Seeking Stomach Cancer Samples
Because the primary treatment for most stages of stomach cancer is surgical resection, stomach cancer samples are likely to be available for stages 0-3, whereas stage 4 stomach cancer samples are less likely to be available because palliative therapies other than palliative surgery make up the primary treatment at that stage. Blood samples may be available as they can be involved in the diagnosis of stomach cancer. Keep in mind, however, that scientists need to be realistic about requesting volumes greater than 1 ml, custom collection protocols, or anything else that deviates from standard care. The more your collection requirements deviate from standard care, the harder the request will be to fill.
For stomach cancer samples or gastric cancer samples collected prospectively, plan ahead as collection times can exceed several months depending on your inclusion and exclusion criteria. Biomarker information is only available if it was collected as part of standard care at the time of treatment. Data mining fees may apply if you require knowledge of specific biomarker criteria that were tested for as part of standard care. Remember that many biorepositories and biobanks contain primarily FFPE samples that have been CAP graduated, which means that elapsed time since the collection procedure often exceeds ten years, and data associated with the samples will reflect standard care as it was a decade ago. Biomarker screening of samples by us is possible, but this is unlikely to be cost effective unless you want to purchase all tested specimens regardless of their biomarker profile. If you only want samples with certain markers, you will have to pay for testing of the ones that are negative too. A better alternative may be to purchase sections only for a statistically suitable number of cases, screen them in your own lab using your preferred assay or a third-party, high volume genetic screening service, then request the blocks of interest.
References
- American Cancer Society (2015). Stomach Cancer. Retrieved from http://www.cancer.org/cancer/stomachcancer/index.
- Bass, A. J., Thorsson, V., Shmulevich, I., Reynolds, S. M., Miller, M., Bernard, B., … Liu, J. (2014). Comprehensive molecular characterization of gastric adenocarcinoma. Nature, 513(7517), 202–209. http://doi.org/10.1038/nature13480
- Cancer.Net (April 2015). Stomach Cancer: Risk Factors. Retrieved from
http://www.cancer.net/cancer-types/stomach-cancer/risk-factors - Gastric Cancer Foundation (2015). Synopsis. Retrieved from http://www.gastriccancer.org/about-
gastric-cancer/what-is-gastric-cancer/synopsis/. - Hamilton, J. P., & Meltzer, S. J. (January 01, 2006). A review of the genomics of gastric cancer. Clinical Gastroenterology and Hepatology: the Official Clinical Practice Journal of the American Gastroenterological Association, 4, 4, 416-25.
- Hudler, Petra. “Genetic Aspects of Gastric Cancer Instability,” The Scientific World Journal, vol. 2012, Article ID 761909, 10 pages, 2012. doi:10.1100/2012/761909.
- Marilanda Ferreira Bellini, Aline Cristina Targa Cadamuro, Maysa Succi, Marcela Alcântara Proença, and Ana Elizabete Silva, “Alterations of the TP53 Gene in Gastric and Esophageal Carcinogenesis,” Journal of Biomedicine and Biotechnology, vol. 2012, Article ID 891961, 13 pages, 2012. doi:10.1155/2012/891961
- Matsueda, S., & Graham, D. Y. (2014). Immunotherapy in gastric cancer. World Journal of Gastroenterology : WJG, 20(7), 1657–1666. http://doi.org/10.3748/wjg.v20.i7.1657
- Milne, A. N., Carneiro, F., O’Morain, C., & Offerhaus, G. J. A. (November 01, 2009). Nature meets nurture: molecular genetics of gastric cancer. Human Genetics, 126, 5, 615-628.
- Mocellin, S., Verdi, D., Pooley, K. A., & Nitti, D. (January 01, 2015). Genetic variation and gastric cancer risk: a field synopsis and meta-analysis. Gut, 64, 8, 1209-19.
- Morano, Federica, Moorcraft, Sing Yu, Chau, Ian. (May 30, 2015). Immunotherapy in Gastric Cancer. American Society of Clinical Oncology. Retrieved from https://am.asco.org/immunotherapy-gastric-cancer.
- Muro K, Bang Y, Shankaran V, et al. (2014) A phase 1b study of pembrolizumab (pembro; MK-3475) in patients with advanced gastric cancer. Annals Onc. Suppl 5:v1-v41.
- National Cancer Institute. (2015a). Gastric Cancer Treatment–for health professionals (PDQ®). Retrieved from http://www.cancer.gov/types/stomach/hp/stomach-treatment-pdq#section/all.
- National Cancer Institute. (2015b). SEER Stat Fact Sheets: Stomach Cancer. Retrieved from http://seer.cancer.gov/statfacts/html/stomach.html.
- Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J., Lortet-Tieulent, J. and Jemal, A. (2015), Global cancer statistics, 2012. CA: A Cancer Journal for Clinicians, 65: 87–108. doi: 10.3322/caac.21262. Retrieved from http://onlinelibrary.wiley.com/doi/10.3322/caac.21262/full
- World Cancer Research Fund International (2015). Stomach Cancer Statistics. Retrieved from
http://www.wcrf.org/int/cancer-facts-figures/data-specific-cancers/stomach-cancer-statistics - Zheng, L., Wang, L., Ajani, J., & Xie, K. (June 01, 2004). Molecular basis of gastric cancer development and progression. Gastric Cancer : Official Journal of the International Gastric Cancer Association and the Japanese Gastric Cancer Association, 7, 2, 61-77.